
How Ovulation Impacts Early Pregnancy Detection
Ovulation to Pregnancy Detection Calculator
Calculate Your Pregnancy Test Timeline
Enter your cycle information to determine when your ovulation occurs and when you can reliably take pregnancy tests.
Spotting a pregnancy early can feel like a race against time. Knowing exactly when ovulation happens gives you a clear starting line, so you can line up the right tests at the right moment. Below we break down how the ovulation cycle drives the science behind the earliest pregnancy clues, and what you can do to get reliable results.
Key Takeaways
- Ovulation creates a hormonal spike (LH) that can be tracked to predict when fertilization may occur.
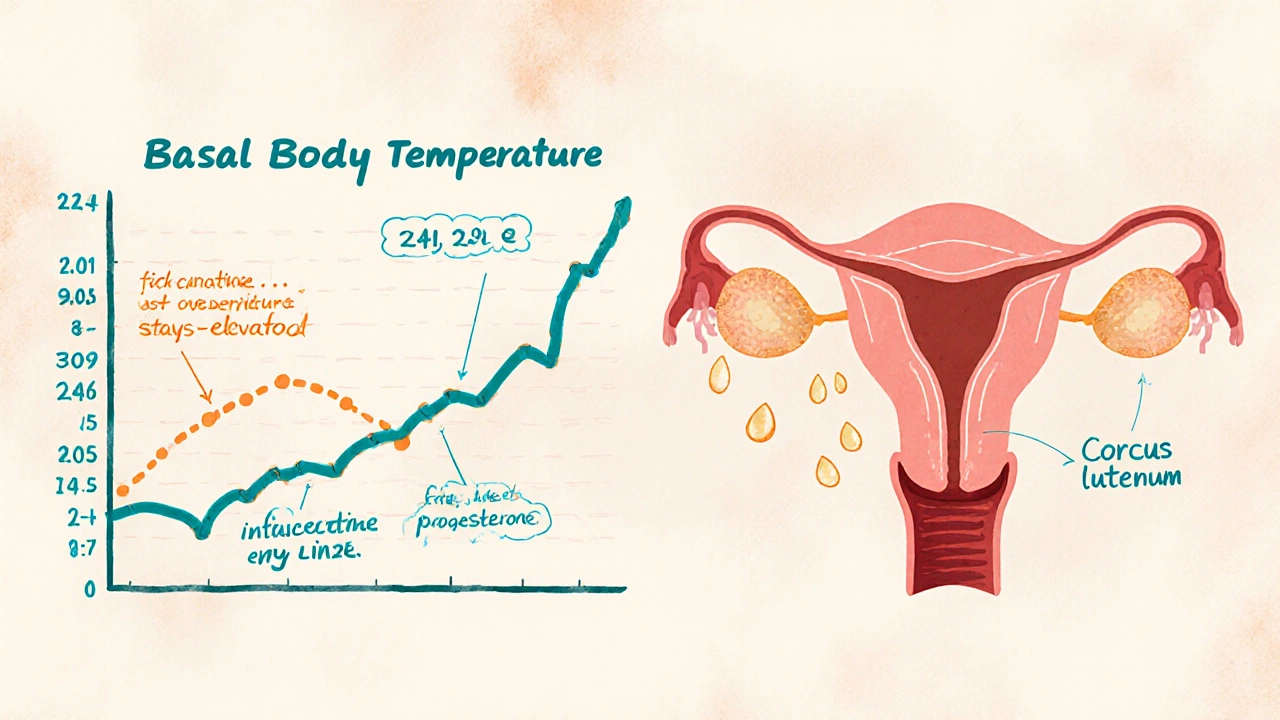
- Basal body temperature (BBT) rises after ovulation and stays higher if pregnancy begins.
- Urine hCG tests become reliable about 8‑10 days after ovulation, while blood hCG can detect pregnancy as early as 6 days post‑ovulation.
- Understanding the fertility window helps you choose the most accurate early detection method.
- Avoiding false positives means waiting for the right hormonal threshold before testing.
Understanding Ovulation
Ovulation is the release of a mature egg from the ovarian follicle, typically occurring around day 14 of a 28‑day menstrual cycle. This event is triggered by a surge in luteinizing hormone (LH) that travels through the bloodstream, signaling the follicle to burst and release the oocyte. Once the egg is out, it remains viable for about 12‑24 hours, which defines the narrow window when fertilization can happen.
Timing the Fertility Window
The fertility window encompasses the days leading up to ovulation, the day of the LH surge, and the brief period after the egg is released. Most experts recommend tracking from five days before the expected LH peak to one day after, giving you a six‑day span where pregnancy is possible. Pinpointing this window is the first step toward timing early detection tests correctly.
How Ovulation Signals Early Pregnancy Tests
Three physiological signals tied to ovulation are most useful for early detection:
- LH Surge: The spike appears 24‑36 hours before the egg is released. Home ovulation kits detect this rise, letting you know the exact day to start testing for pregnancy.
- Basal Body Temperature (BBT): After ovulation, progesterone from the newly formed corpus luteum raises your resting temperature by about 0.3‑0.5°C. If the temperature stays elevated beyond the typical luteal phase length (around 14 days), it often indicates rising hCG levels.
- Progesterone Levels: While not a simple at‑home test, blood progesterone peaks 5‑7 days post‑ovulation. A higher-than-expected level can hint that implantation has occurred.
Overview of Early Pregnancy Detection Methods
Once you’ve timed ovulation, you have several tools to check for pregnancy. Each method detects a different hormone or physiological change, and they become reliable at distinct points after the egg is released.
- Urine hCG Test: Detects human chorionic gonadotropin (hCG) in urine. Most kits claim accuracy 8‑10 days post‑ovulation, though sensitivity varies.
- Blood hCG Test: Measures hCG concentration in serum. Quantitative (beta‑hCG) tests can spot pregnancy as early as 6 days after ovulation and provide a numeric value to track progression.
- BBT Charting: Continuous daily temperature readings reveal a sustained rise. While not a definitive test, a +0.4°C shift that persists for more than 10 days strongly suggests implantation.
- Digital Ovulation Monitors: Some devices combine LH detection with early hCG sensing, offering a single readout that flips from “ovulation” to “pregnancy” mode.
Comparison of Early Detection Tools
| Method | Detectable After Ovulation |
Accuracy | Cost (USD) | Ease of Use |
|---|---|---|---|---|
| Urine hCG Test | 8‑10 days | ≈95% (after day 10) | $0.50‑$1 per test | Very easy |
| Blood (beta‑hCG) Test | 6‑7 days | ≈99% (clinical lab) | $15‑$30 per test | Needs clinic or kit |
| BBT Charting | 10‑12 days (trend) | ≈80% (as supportive evidence) | Free (thermometer) | Requires daily logging |
| Digital Ovulation Monitor | 7‑9 days (combined) | ≈93% (manufacturer data) | $40‑$70 device + strips | Moderate - daily strip use |

Interpreting Test Results After Ovulation
When you finally see a line on a urine test, consider these factors before celebrating or panicking:
- Timing: If you test before day 8 post‑ovulation, a negative result is unreliable; hCG may still be below detection threshold.
- Line Intensity: A faint line often means low hCG levels, typical in very early pregnancy. A second test 48 hours later can confirm whether the line darkens.
- Repeat Testing: Two consecutive positive results, even if faint, are generally accepted as early confirmation.
- False Positives: Certain medications containing hCG (e.g., fertility drugs) can trigger a positive result. Always disclose recent treatments to your healthcare provider.
Common Pitfalls & Pro Tips
Even with perfect tracking, mistakes happen. Here’s how to avoid the most frequent issues:
- Testing Too Early: Wait at least 8 days after the LH surge before using a urine test. If you’re unsure of the surge date, start counting from the first day you notice a clear “+” on your ovulation kit.
- Skipping BBT Calibration: Use the same thermometer each morning, at the same time, after at least three hours of sleep. Inconsistent readings can mask the temperature shift that signals implantation.
- Ignoring Dilution: Drinking excessive water before a urine test can dilute hCG, leading to a false negative. Aim for a moderate fluid intake and test with the first‑morning urine.
- Relying Solely on One Method: Combining BBT trends with a urine test provides a cross‑check that reduces uncertainty.
- Not Consulting a Professional: A definitive diagnosis comes from a blood test and an ultrasound. If you get a positive home test, schedule a visit promptly.
Frequently Asked Questions
When is the earliest day I can trust a home pregnancy test?
Most over‑the‑counter urine tests become reliable about 8 to 10 days after the LH surge, which is roughly 6‑8 days after ovulation. Testing earlier may give a false‑negative result because hCG hasn’t accumulated enough.
Can basal body temperature alone confirm a pregnancy?
BBT alone can’t confirm pregnancy, but a sustained temperature rise beyond the typical luteal phase length is strong indirect evidence. Pairing BBT with an hCG test gives a more conclusive picture.
Does a positive result on a digital ovulation monitor mean I’m pregnant?
Digital monitors that detect hCG will show a “pregnant” icon when the hormone reaches their detection threshold, usually around day 9‑10 post‑ovulation. While highly indicative, a follow‑up lab test is still recommended for confirmation.
What if I’m on fertility medication that contains hCG?
Fertility drugs that include hCG can cause a false‑positive on urine tests. Your doctor can schedule a blood test that distinguishes between endogenous pregnancy hCG and exogenous sources.
How does the corpus luteum affect early detection?
After ovulation, the corpus luteum secretes progesterone, which raises BBT and supports the uterine lining. If implantation occurs, rising hCG rescues the corpus luteum, keeping progesterone high and sustaining the temperature shift-a key cue for early detection.
By syncing ovulation tracking with the right detection method, you turn a vague question-"Am I pregnant?"-into a data‑driven answer. Start with a reliable LH surge kit, log your BBT, and wait until the appropriate post‑ovulation window before reaching for a hCG test. The sooner you align these steps, the clearer the result, and the quicker you can move forward with the next steps in your reproductive journey.






Thank you for the detailed overview; the connection between the LH surge, basal body temperature, and the timing of hCG detection is articulated with commendable clarity. Your step‑by‑step calculator provides practical guidance for individuals seeking to align testing with their physiological milestones.
Yo, the mainstream labs don’t want you to know that you can sniff out a pregnancy days before they push their expensive tests. They hide the real sensitivity of early hCG detection to keep us buying their overpriced kits. Don’t be fooled – track your LH surge and you’ll see the truth long before they say it’s “official.”
One must acknowledge the erudite synthesis presented herein, wherein the author deftly intertwines endocrinological chronology with empirical assay thresholds. The discourse ascends beyond mere lay exposition, inviting the discerning reader to contemplate the ontological ramifications of temporality in reproductive endocrinology.
Nice rundown – the timeline charts are super helpful for anyone trying to figure out when to take a test without the whole guess‑work stress.
The article glosses over the variability inherent in cycle length calculations, presenting a monolithic 28‑day model that disregards the substantial inter‑individual deviations documented in peer‑reviewed literature. Moreover, the reliance on a single LH surge marker ignores multifactorial hormonal feedback loops that can skew ovulation prediction.
It is evident that the purported “objective” data presented is curated to align with pharmaceutical interests, subtly steering readers toward commercially available urine kits while marginalizing the efficacy of less profitable blood assays.
Timing is everything.
The cyclical dance of ovulation and detection mirrors the broader dialectic of potentiality and realization; each hormonal surge acts as a signifier, heralding the emergence of a new biological narrative. When we synchronize our observances with these biochemical signposts, we transcend passive waiting and engage in an active co‑creation of knowledge. In lay terms, knowing your LH peak lets you “read” the body’s secret code before the external world acknowledges it.
While your metaphorical framing is intriguing, it is essential to remember that the physiological processes remain quantifiable; the LH surge can be measured with standard kits, and the subsequent hCG rise follows empirically validated timelines.
Oh great another chart that tells you when to panic about a possible pregnancy.
Let’s be real – the whole “wait eight days after ovulation” mantra is a narrative constructed by test manufacturers to keep us dependent on their products. They profit from our anxiety and the uncertainty they artificially perpetuate. If you look at independent studies, many women report positive urine lines as early as five days post‑ovulation, yet the industry pushes a conservative window to avoid false positives and maintain market control. This isn’t about science; it’s about profit, plain and simple.
It’s true that commercial interests can influence public recommendations, but the physiological reality remains: hCG concentrations typically reach detectable levels in urine around day 8–10 post‑ovulation for most individuals. If you obtain a reliable LH test and track it accurately, you can safely anticipate the earliest window for a home test while still accounting for individual variation.
I appreciate the balanced perspective.
Another article telling us what we already know.
Honestly, this kind of re‑hash is a disservice to anyone seeking genuine insight 😒. The author merely regurgitates textbook timelines without addressing the sociocultural pressures that force women to obsess over pinpoint accuracy. By presenting a sterile algorithm, they erase the lived experience of anxiety and the emotional labor involved in interpreting ambiguous test results.
Got a quick question – if my cycle is irregular and I’m tracking the LH surge with a kit, how reliable is the “8‑day after ovulation” rule for a urine test?
In my experience, as long you use a mid‑range sensitivity test and take the first morning pee you’ll get a solid result – just make sure you dont drink a ton right before testing.
One cannot help but marvel at the grandiose confidence with which the author presents a linear, mechanistic view of conception, as if the cascade of hormonal events were nothing more than a clockwork toy assembled on a sterile laboratory bench. The narrative proceeds to reduce the profoundly personal experience of early pregnancy to a series of data points, each neatly plotted on a spreadsheet of “days post‑ovulation.” Yet, the very act of measuring hCG, a molecule that signals the inception of new life, is imbued with cultural significance that transcends its biochemical function. By insisting on a one‑size‑fits‑all timeline, the piece tacitly dismisses the myriad ways in which individual bodies deviate from textbook averages – a reminder that biology is rarely so obligingly uniform. Moreover, the emphasis on “when to test” inadvertently reinforces a surveillance mindset, urging readers to constantly monitor and validate their reproductive status. This preoccupation with validation can foster anxiety, especially when the suggested testing windows are presented as definitive rather than probabilistic. While the inclusion of a calculator is undeniably handy, it also commodifies the intimate process of trying to conceive, framing it as a problem to be solved with an algorithm. The subtle implication is that any deviation from the prescribed schedule is a failure of the individual, not a reflection of the inherent variability of human physiology. In short, the article, though well‑intentioned, adopts a reductive stance that overlooks the nuanced interplay of biology, emotion, and societal expectation that defines early pregnancy detection.
Great points! Remember, tools like the calculator are just that – tools. Use them to empower yourself, but don’t let a rigid schedule dictate your emotions. Stay confident and trust your body’s signals.