Opioid-Induced Constipation: How to Prevent and Treat It Effectively
More than half of people taking opioids for chronic pain develop constipation - and it doesn’t go away on its own. Unlike the nausea or drowsiness that might fade after a few days, opioid-induced constipation (OIC) sticks around as long as you’re on the medication. It’s not just uncomfortable; it can lead to bloating, nausea, vomiting, and even dangerous blockages if left untreated. Yet, many patients and even some doctors treat it as a normal side effect instead of a medical problem that needs active management.
Why Opioids Cause Constipation
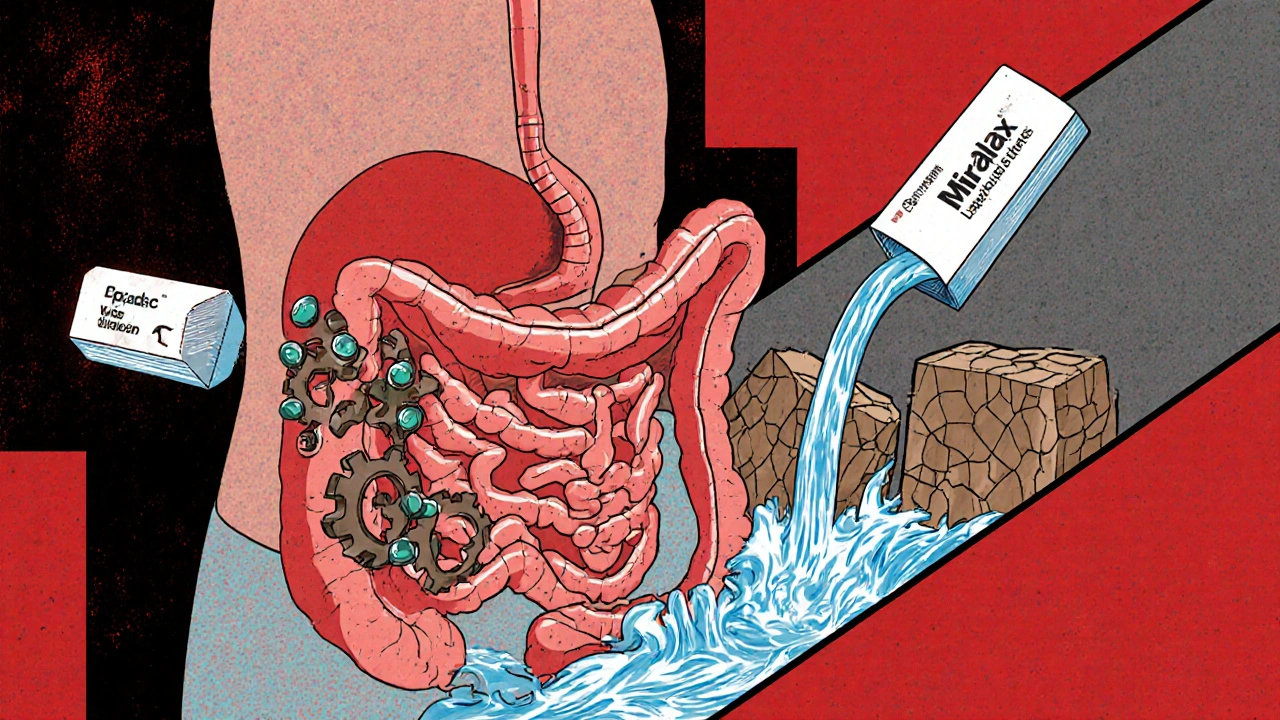
Opioids don’t just block pain signals in your brain. They also bind tightly to receptors in your gut, slowing everything down. This isn’t just about reduced bowel movements - it’s a full-system shutdown. The muscles in your intestines relax, so food moves slower. Water gets sucked out of your stool, making it hard and dry. Your anal sphincter tightens, making it harder to push out even when you feel the urge. This is why typical constipation remedies often fail. You can’t fix this with just more fiber or water. The problem is rooted in how opioids change your nervous system’s control over digestion.Studies show that 40% to 60% of people on long-term opioids for non-cancer pain develop OIC. For cancer patients in hospice or palliative care, that number jumps to 70% to 100%. It can start within days of beginning opioid therapy - or creep up slowly over weeks. Either way, if you’re on opioids and not pooping regularly, it’s likely OIC.
Prevention Is the Best Strategy
Waiting until you’re straining to start treatment is a mistake. Experts agree: you should begin laxatives the same day you start opioids. This simple step prevents severe constipation in 60% to 70% of cases. Yet, too many patients are left to figure it out on their own. Pharmacists who proactively recommend bowel regimens when filling opioid prescriptions increase proper laxative use by 43%.Start with a daily osmotic laxative like polyethylene glycol (Miralax). It pulls water into the colon without irritating the bowel lining. Add a stimulant laxative like senna or bisacodyl if you need more push. Don’t rely on stool softeners like docusate alone - they don’t do enough for OIC. Drink plenty of water, stay active, and eat fiber-rich foods, but understand: lifestyle changes alone won’t fix this. You need targeted medication from day one.
First-Line Treatments: What Works (and What Doesn’t)
Most people try over-the-counter laxatives first. But here’s the catch: standard constipation meds often fail for OIC because the cause is different. Stimulant laxatives (senna, bisacodyl) and osmotic agents (PEG) are the only OTC options with solid evidence for OIC. Enemas and suppositories can help with acute blockages but aren’t for daily use.Here’s what patients report on pain forums: 68% say OTC laxatives give them only partial relief. Many describe spending hours on the toilet, still feeling incomplete. That’s not normal - it’s a sign you need stronger help.

Prescription Options: PAMORAs Are Game-Changers
When laxatives aren’t enough, the next step is PAMORAs - peripherally acting μ-opioid receptor antagonists. These drugs block opioids from acting in your gut but can’t cross into your brain, so your pain relief stays intact. They’re not magic pills, but they’re the most effective solution for persistent OIC.There are four FDA-approved PAMORAs:
- Methylnaltrexone (Relistor®): Given as a daily injection or now a once-weekly shot. Works in as little as 30 minutes. Often used in advanced illness or palliative care.
- Naldemedine (Symproic®): Once-daily pill. Proven to improve bowel function and may reduce opioid-induced nausea too. Recommended by ASCO for cancer patients starting opioids.
- Naloxegol (Movantik®): Daily tablet. Works well for chronic noncancer pain patients.
- Lubiprostone (Amitiza®): Not a PAMORA - it activates chloride channels to increase fluid in the gut. FDA-approved for women, but effective in men too. Can cause nausea in 1 out of 3 users.
Patients on Reddit and PatientsLikeMe report dramatic improvements: "Relistor worked when nothing else did," one wrote. "Naldemedine let me stay on my pain meds without constant bathroom struggles," said another. But it’s not perfect. About 28% report abdominal pain as a side effect. And cost is a huge barrier - $500 to $900 a month without insurance.
The Hidden Risks
PAMORAs are powerful, but they come with serious warnings. They’re absolutely not safe if you have a bowel obstruction or are at risk for one - like after recent abdominal surgery or with severe inflammatory bowel disease. There have been documented cases of life-threatening bowel perforation linked to these drugs. The FDA requires special patient education and provider training because of this risk.Don’t take them if you’re bloated, have severe cramping, or haven’t had a bowel movement in days without medical guidance. Always tell your doctor about any history of gut surgery, diverticulitis, or Crohn’s disease.

Why So Many People Still Suffer
Despite clear guidelines, OIC remains massively undertreated. Only 32% of primary care doctors start bowel regimens when prescribing opioids. In hospice settings, it’s 85%. Why the gap? Patients are reluctant to add more pills. Doctors assume it’s "just constipation." Insurance companies make access hard - 41% of Medicare Part D plans require prior authorization for PAMORAs. Some require you to fail three OTC laxatives first, even though guidelines say that’s ineffective.Patients often stop PAMORAs within six months - not because they don’t work, but because they’re too expensive or don’t get full relief. A 2023 survey found 57% discontinued them due to cost or limited effectiveness. That’s a failure of the system, not the medication.
What’s Next for OIC Treatment
The future is promising. A once-weekly version of methylnaltrexone is already here, reducing injection burden. Researchers are testing combination pills that pair low-dose PAMORAs with gentle laxatives for better results. And by 2026, doctors may use genetic testing to predict which patient responds best to which drug - personalizing treatment instead of guessing.Meanwhile, the American Society of Gastroenterology says poor OIC management costs the U.S. $2.3 billion a year in ER visits, hospitalizations, and lost productivity. That’s why they’re pushing insurers to cover evidence-based treatments without unnecessary barriers.
What You Should Do Right Now
If you’re on opioids and constipated:- Don’t wait. Start polyethylene glycol (Miralax) daily and senna at night.
- Talk to your doctor about PAMORAs if you’re still struggling after 1-2 weeks.
- Ask your pharmacist to review your full regimen - they’re trained to spot OIC.
- Track your bowel movements using the Bowel Function Index (BFI). A score above 30 means you need treatment change.
- If you have cancer or are in palliative care, ask about naldemedine - it’s specifically recommended for you.
Constipation from opioids isn’t something you have to live with. It’s treatable. But only if you speak up, ask for help, and don’t accept "it’s normal" as an answer. Your quality of life matters more than your fear of adding another pill.
Can opioid-induced constipation go away on its own?
No. Unlike other opioid side effects like drowsiness or nausea, which often improve after a few days, opioid-induced constipation (OIC) persists as long as you’re taking the medication. It’s caused by a direct effect on gut nerves, not temporary inflammation or sensitivity. Without treatment, it typically worsens over time.
Are over-the-counter laxatives enough for opioid-induced constipation?
For many people, no. While osmotic laxatives like polyethylene glycol and stimulants like senna are recommended as first-line treatments, studies show 68% of patients still have inadequate relief. OIC has a unique mechanism - opioids physically slow gut movement - so standard constipation remedies often fall short. If OTC options aren’t working after 1-2 weeks, it’s time to talk to your doctor about prescription options like PAMORAs.
What are PAMORAs and how do they work?
PAMORAs - peripherally acting μ-opioid receptor antagonists - block opioids from binding to receptors in your gut, restoring normal bowel movement without affecting pain relief. Because they can’t cross the blood-brain barrier, they don’t interfere with the pain-killing effects of your opioid. Examples include methylnaltrexone (Relistor®), naldemedine (Symproic®), and naloxegol (Movantik®). They’re the most effective treatment for persistent OIC.
Is it safe to use PAMORAs if I’ve had abdominal surgery?
No. PAMORAs are contraindicated if you have a known or suspected bowel obstruction, recent abdominal surgery, or conditions like Crohn’s disease or diverticulitis. These drugs increase gut motility, which can cause dangerous perforations in weakened or inflamed tissue. Always tell your doctor about your surgical history before starting any PAMORA.
Why are PAMORAs so expensive?
PAMORAs are brand-name drugs with no generic equivalents yet, and they’re priced between $500 and $900 per month without insurance. Insurance companies often require prior authorization or step therapy - forcing you to try cheaper laxatives first, even though guidelines say that’s ineffective. Some patients drop out due to cost, even when the drugs work. Patient assistance programs and manufacturer coupons can help reduce out-of-pocket costs.
Can I prevent opioid-induced constipation without medication?
Diet and lifestyle help, but they’re not enough on their own. Drinking water, eating fiber, and staying active support bowel health - but opioids override these efforts by directly slowing gut nerves. Prevention requires starting a laxative regimen on day one of opioid therapy. Waiting until you’re constipated means you’re already behind.
What should I do if my current laxative isn’t working?
Don’t increase the dose indefinitely. If you’ve been on standard laxatives for 1-2 weeks with no improvement, schedule a follow-up with your doctor. Ask about PAMORAs. Use the Bowel Function Index (BFI) to track your symptoms - a score above 30 means you need a stronger approach. Your doctor may switch you to a different laxative class or add a PAMORA. Escalation is necessary - not a failure.
Do PAMORAs work for cancer patients?
Yes - and they’re specifically recommended for this group. The American Society of Clinical Oncology (ASCO) 2024 guidelines state that naldemedine (Symproic®) should be considered for cancer patients starting regular opioid therapy. It improves bowel function and may also reduce opioid-induced nausea and vomiting. For patients in palliative care, methylnaltrexone injections are often used because they act quickly and reliably.
How do I know if I have opioid-induced constipation or just regular constipation?
If you started opioids recently and now have straining, hard stools, or a feeling of incomplete evacuation - especially if OTC remedies aren’t helping - it’s likely OIC. Regular constipation improves with fiber and fluids. OIC doesn’t. It’s persistent, worsens with continued opioid use, and often requires prescription intervention. If you’re unsure, ask your doctor to use the Bowel Function Index (BFI) - a simple tool that scores your symptoms.
What’s the long-term outlook for managing opioid-induced constipation?
With proper management, most people can maintain regular bowel function while staying on their pain medication. The key is early, proactive treatment. As new formulations (like once-weekly injections) and personalized approaches emerge, treatment will become easier and more accessible. The real challenge isn’t medical - it’s access. Insurance barriers and lack of provider awareness still leave many suffering unnecessarily. But you’re not alone - effective options exist, and you deserve relief.





why do people still think fiber fixes this? opioids dont care about your kale smoothie. its a neurologic blockade not a dietary deficiency. if you’re still straining after miralax and senna, you’re not trying hard enough.
OMG I CANT BELIEVE THIS IS STILL A THING. I WAS ON OXYCODONE FOR 6 MONTHS AND MY DOCTOR SAID JUST "EAT MORE BRAN" LIKE I WAS A 70-YEAR-OLD WITH A SLOW DIGESTION. I HAD TO GO TO THE ER BECAUSE I WAS BLOCKED. THEN I FOUND OUT ABOUT RELISTOR AND IT WAS LIKE GOD SPOKE TO ME. WHY IS THIS NOT STANDARD???
I just wanted to say thank you for writing this. I’ve been on long-term opioids for fibromyalgia and no one ever told me to start laxatives right away. I wish I’d known sooner. I spent months feeling like my body was betraying me. Now I’m on naldemedine and honestly? I feel like myself again. It’s not glamorous, but it’s life-changing.
soooooo... lets get this straight... youre telling me that people who take pain meds are just... too lazy to poop?? and now we need fancy $800 pills?? i mean cmon. my grandpa took morphine in the 80s and he just ate prunes. no big deal. weve gotten soft. also why is everyone so obsessed with this? its just constipation. get over it.
gordon. you’re the reason people hate this system. i had a bowel obstruction from OIC and you think prunes fix it? i had to get a colostomy bag for 3 months. this isn’t about being soft. its about medical neglect. stop being a jerk.
Just wanted to add that pharmacists are seriously underrated here. My pharmacist flagged my opioid script and gave me a free sample of Miralax with a printed guide. That small act saved me from months of suffering. If your doc doesn’t mention it, ask your pharmacist. They’re trained for this.
Thanks for the detailed breakdown. I’ve been on naldemedine for 8 months and it’s been a game-changer. I’m not saying it’s perfect-sometimes I get cramps-but compared to the agony before? No contest. I wish more doctors knew how to explain this without making patients feel guilty.
OIC is not a problem it is a signal. The body is asking for balance. Modern medicine tries to fix symptoms with pills. But true healing comes from understanding the root. Opioids are a tool. The gut is a temple. We must respect both.
Oh please. "PAMORAs are game-changers"? Sure. Until you realize they’re just opioid blockers with a fancy acronym. And yes, they cost a fortune. But here’s the real scandal: Big Pharma invented this problem to sell $900 pills. You think they’d let you fix constipation with Miralax? Please. They need you dependent on their $700/month miracle. This is capitalism disguised as medicine.
Let me tell you what happened to my cousin. She was on fentanyl for endometriosis. Started Miralax. Didn’t work. Tried senna. Still nothing. Then she got Relistor. Within 17 minutes? She had her first normal bowel movement in 11 weeks. She cried. I cried. We all cried. This isn’t just medicine. This is dignity. This is freedom. This is the difference between living and just existing.
How ironic that the same society which glorifies stoicism in pain management pathologizes the natural consequence of its own pharmacological tyranny. The gut, as the second brain, is silenced by the opioid’s hegemony over mu-receptors-yet we expect patients to endure this as if it were a rite of passage. The pharmaceutical-industrial complex profits from this silent suffering, while doctors, blinded by protocol, prescribe laxatives like they’re offering a cup of tea at a funeral. We are not treating constipation-we are appeasing a system that commodifies bodily autonomy.
My dad’s a Vietnam vet on long-term opioids. He never knew about PAMORAs until I found this article. We called his VA doctor. They approved naldemedine in two days. He’s pooping regularly for the first time in 12 years. This isn’t just medical info-it’s a lifeline. Thank you for writing this. More people need to see it.